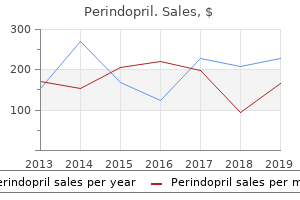
"Buy generic perindopril 8mg, blood pressure medication name brands".
By: Z. Trano, M.B.A., M.B.B.S., M.H.S.
Associate Professor, Johns Hopkins University School of Medicine
Induction of in vivo insulin resistance by hyperglycemia In type 1 diabetic sufferers lacking endogenous insulin secretion arrhythmia quiz cheap 8mg perindopril mastercard, results of hyperglycemia per se on insulin action may be examined hypertension differential diagnosis cheap 2mg perindopril overnight delivery. These dose-response curves were created in people by inhibiting endogenous insulin secretion with somatostatin in wholesome volunteers and by then increasing glucose and insulin concentrations to desired levels on separate days heart attack normal ekg purchase perindopril 2mg line. Doubling the plasma glucose focus from 5 to 10 mmol L-1 significantly increases the speed of glucose uptake arteria3d unity perindopril 2 mg free shipping. The mass-action impact of glucose depends upon the ambient insulin concentration and is far larger at postprandial than fasting insulin concentrations. Glucose toxicity 415 30 mmol L1 Plasma glucose Glucose extraction Blood move 30 three. Plasma glucose and serum free insulin concentrations throughout a normoglycemic day, and through a hyperglycemic day induced by infusion of glucose. After each examine day, the speed of glucose uptake throughout the forearm was measured underneath standardized conditions of glycemia and insulinemia to quantitate insulin sensitivity. Preceding hyperglycemia considerably decreased glucose extraction but had no impact on blood flow. Animal models, nevertheless, gave clearer proof of the primacy of glucose on this phenomenon. In the rat, for example, removal of 90% of the pancreas causes insulin deficiency, hyperglycemia, and a 30% discount in insulin-stimulated glucose utilization in skeletal muscle [5]. These studies along with the human information supplied the primary proof of the flexibility of the blood glucose concentration itself to regulate insulin sensitivity, and the phenomenon began to be referred to as "glucose toxicity" [7,20]. Hyperglycemia as a mediator of insulin resistance in kind 2 diabetes In sort 2 diabetes, a lot of studies are according to the glucose toxicity idea though interpretation of those research is sometimes not so simple as the research of type 1 diabetes due to the complicated pathophysiology of sort 2 diabetes. It might be argued, due to this fact, that any remedy that makes a subject more insulin delicate will in the end decrease insulin ranges, making them extra insulin delicate through that mechanism alone. Nevertheless, the data obtainable are at 50 Rate of glucose uptake (mg kg1 min1) forty 30 20 10 zero 02 h 57 h mL dL min1 zero 250 2. Garvey and coworkers, for example, demonstrated that three weeks of intensive insulin therapy significantly improved the maximum glucose disposal price, endogenous glucose output, and insulin secretory capability [24], and comparable findings were also obtained in different laboratories [25]. The fact that basal insulin ranges were unchanged in the weight reduction study [23] and increased after intensive insulin therapy [24] suggest that insulinemia per se was not the driving pressure for the modifications in insulin sensitivity. Furthermore, other therapeutic interventions similar to sulfonylureas additionally improve insulin sensitivity, consistent with 416 Chapter 27 the idea that glucose was a principal driver of the insulin resistance prior to remedy. Since that time, additional support for this idea has been obtained from all kinds of in vitro and in vivo fashions, a few examples of which observe. The in vitro studies are significantly compelling due to the power to isolate glucose as a dependent variable. Insulin-stimulated glucose transport in muscle strips of hyperglycemic kind 2 diabetic sufferers was lower than that of normoglycemic subjects however extended exposure to normoglycemia fully reversed that defect [26]. Isolated adipocytes additionally respond to high concentrations of glucose by desensitizing their glucose transport system [27]. Physiologic basis of glucose-induced insulin resistance in vivo In insulin-treated sufferers with kind 1 diabetes, in whom glucose toxicity appears to be the most important reason for insulin resistance, direct quantitation of tissue glucose uptake throughout insulin stimulation utilizing positron emission tomography has demonstrated that skeletal muscle is the predominant tissue responsible for the defect in insulin-stimulated glucose utilization [28]. Since a substantial fraction of whole-body glucose oxidation is unbiased of insulin, rates of whole-body glucose oxidation should be corrected for the estimated contribution of this element of glucose oxidation [29]. When this is accomplished in sufferers with type 1 [12] or type 2 [30] diabetes, the fractions of glucose oxidized and disposed of nonoxidatively (the sum of glycogen synthesis and nonoxidative glycolysis) are just like those in regular topics. These information suggest that whatever the main mobile course of causing insulin resistance, the ultimate gate-keeper for cellular glucose uptake is located at the stage of glucose transport or phosphorylation. In support of this, muscle glucose-6-phosphate concentrations are comparable in insulin-resistant patients with sort 1 diabetes underneath circumstances the place glucose flux is acutely normalized by hyperglycemia beneath hyperinsulinemic conditions as beneath conditions of normoglycemic hyperinsulinemia [12]. Another hypothetical possibility is that glucose supply could possibly be rate-limiting for glucose disposal. Insulin, at physiologic concentrations, will increase blood circulate, depending on factors similar to limb muscularity and physical fitness from -10 to 80% (mean in 75 research around 20%) [33]. Although defects in blood flow may be noticed at supraphysiologic insulin concentrations in patients with sort 1 or sort 2 diabetes, research performed at physiologic insulin concentrations locate impaired insulin motion solely to glucose extraction [33]. Taken collectively these data localize hyperglycemia-induced insulin resistance of glucose utilization to early steps in glucose uptake in skeletal muscle. This defect is accompanied by comparable relative reductions in glucose oxidation and storage. Chronic hyperglycemia as a explanation for impaired insulin secretion In 1948, Lukens and Dohan administered large doses of glucose to normal cats and induced everlasting hyperglycemia, hydropic degeneration of the islet of Langerhans, and ketonuria in 4 out of 35 cats studied [34].
Cytosolic phosphoenolpyruvate is converted to fructose-1 blood pressure standards buy perindopril now,6bisphosphate by way of six enzymatic steps common to glycolysis arrhythmia specialist 8 mg perindopril visa. Fructose-6-phosphate is then converted to glucose-6-phosphate by reversal of the hexose phosphate isomerase response of glycolysis lennox pulse pressure test kit buy perindopril without a prescription. The terminal step of gluconeogenesis is the hydrolysis of glucose-6-phosphate (G6P) to free glucose blood pressure log sheet printable buy discount perindopril on line, catalyzed by the glucose-6-phosphatase (G6Pase) enzyme complicated. Specificity of the system is conferred by the T1 translocase part, which transports glucose-6-phosphate, however not its closely related epimer mannose-6-phosphate. Classic glucoregulatory hormones similar to insulin, glucagon, and glucocorticoids mediate gluconeogenic gene expression by promoting or inhibiting the interplay of those proteins with the promoter regions of those genes [23]. The stability of this advanced is modulated by way of phosphorylation of the interacting domains by a quantity of kinases, including Ca2+ /calmodulin-dependent kinases [21]. Insulin and counterregulatory hormones instigate transcriptional occasions that modify the expression of key gluconeogenic enzymes. Other factors such as glucocorticoids even have nuclear receptors that induce expression of gluconeogenic enzymes. These events set off a broader phosphorylation cascade which mediates the metabolic impact of insulin. Acute regulation of gluconeogenesis Prior to discovery of the transcriptional mechanisms described earlier, the management of hepatic glucose metabolism was examined in great element on the idea of substrate, allosteric, and posttranslational modification. These factors alter gluconeogenic flux rapidly (seconds to minutes) and are a critical first response to elevated glucose demand. Much of the acute regulation of gluconeogenesis is predicated on the antithetic regulation of a quantity of gluconeogenic/glycolytic enzyme pairs that catalyze opposing pathways. Allosteric binding websites are separate from the catalytic domains and interact with their effector molecules by noncovalent bonding. Typically, electrostatic or hydrogen bonding between the effector molecule and amino acid residues of the allosteric binding pocket cause a change in the quaternary structure of the protein or otherwise change the binding fixed of the catalytic website of the enzyme. Importantly, the effect on conformation and exercise is essentially instantaneous and independent of the transcriptional mechanisms described earlier. In contrast, covalent modification happens when new useful teams are added to amino acids of the enzyme. The effect of covalent modification also modifications the conformation and therefore the exercise of the enzyme. The most typical forms of covalent modifications of metabolic enzymes are phosphorylation and acetylation, although many others also can occur. Covalent modification requires the exercise of other proteins corresponding to kinases and/or phosphorylases to add or cleave covalently bound functional teams. These divergent fates of pyruvate are influenced by dietary state and are reciprocally regulated by allosteric and or covalent modification. Acetyl-CoA then again is a robust allosteric activator of pyruvate carboxylase. Thus high energy states facilitate gluconeogenesis and suppress glucose oxidation and/or lipogenesis. The Ka for acetyl-CoA binding is 2060 uM, a worth within the biologic vary of acetyl-CoA focus in liver mitochondria [35]. Collectively these pathways are referred to as pyruvate biking, and ostensibly confer greater metabolic flexibility by directing an already active flux in the course of or away from gluconeogenesis on fast time scales [15]. Fructose-1,6-bisphosphatase/ phosphofructokinase Allosteric regulation of hexose flux is another example where the regulation of gluconeogenesis happens by interplay with glycolytic regulation. The conversion of F-1-P to F-1,6-P2 is irreversibly catalyzed by the gluconeogenic enzyme fructose-1,6bisphosphatase, and the alternative glycolytic response is irreversibly catalyzed by phosphofructokinase. More importantly, phosphofructokinase is regulated by F-2,6-P2, a product of F-1,6-P2 and the bifunctional enzyme. Fructose-1,6-bisphosphatase can be inhibited by F-2,6-P2, the product of the bifunctional enzyme throughout feeding [15]. Hepatic energetics and glucose production Hepatic gluconeogenesis makes use of greater than 40% of the vitality consumed by the human liver [36]. Consequently, fat oxidation is required for optimal gluconeogenesis in hepatocytes and perfused liver [44]. When defects in fats oxidation happen, both as a result of focused ablation in mice or inborn errors in people, impaired gluconeogenesis and hypoglycemia almost at all times emerge as complications.
Another mechanism by which triglycerides can accumulate is defective lipolysis inside hepatocytes blood pressure chart normal perindopril 8mg with visa. In overweight subjects arteria tapada en ingles order perindopril 4mg mastercard, a decrease in serum adiponectin is more likely to arteria glutea superior order perindopril in united states online contribute to fats accumulation in the liver and may induce hepatic irritation and insulin resistance (see [28] for review) blood pressure going up and down buy generic perindopril 4mg on line. The change in intestinal bacterial flora is thought to alter the permeability of gut mucosa to inducers of irritation corresponding to endotoxin. Over 50 years ago, Jean Vague categorized obese topics in accordance with the diploma of "masculine differentiation" [31] into those with "gynoid" and those with "android" obesity. Gynoid weight problems was characterized by lower-body deposition of fat (around the thighs and buttocks, "pear-shaped") and relative underdevelopment of the musculature, while android weight problems defined upper-body (truncal, "apple-type") adiposity, greater general muscular growth and a bent to develop hypertension, diabetes, atherosclerosis, and gout. These phenotypic observations have subsequently been confirmed in plenty of cross-sectional and potential research (see [32] for review). The quantity of visceral fats correlates carefully with the quantity of fats within the liver [3]. Visceral fats may release extra inflammatory cytokines than subcutaneous adipose tissue [32]. If overactive lipolysis were responsible for the dangerous results of visceral fats, one would predict this depot to be lowered quite than enlarged. Patients with the polycystic ovary syndrome are extra insulin resistant and have a higher liver fat content material than equally overweight topics with out the syndrome [40]. It produces exclusively saturated fatty acids [43], which relative proportion in the liver [44], as nicely as price of production will increase in direct proportion to liver fat in people [45]. Some of fructose may be metabolized within the colon and influence intestine microbiome [46]. In a small (n = 12) but fastidiously carried out mechanistic study, exercising 3060 min 5 times per week for 16 weeks modestly decreased liver fat by 10% within the absence of adjustments in physique weight [52]. The impact of train seems small in comparison to the results of a hypocaloric ketogenic food plan; when the identical group followed a low carbohydrate diet, liver fat was proven to lower by 30% inside forty eight hours [53]. This variant was found in 2008 in a genome-wide affiliation scan in Hispanic, African American, and European American individuals. In a meta-analysis comprised of sixteen research revealed in 2011, homozygous carriers of the variant as compared to noncarriers had a 73% larger lipid fat content, a 3. These data suggest that the I148M substitution is a loss-of-function mutation impairing triglyceride hydrolysis. This familial clustering is observed even after adjusting for age, gender, and weight problems [55]. Nondiabetic hyperglycemia and hyperinsulinemia are well established predictors of sort 2 diabetes. Once fatty, the ability of insulin to inhibit glucose production is impaired, which stimulates insulin secretion leading to hyperinsulinemia. For these topics, liver fat content is a wonderful marker of the metabolic abnormalities characterizing the MetS. International Journal of Obesity and Related Metabolic Disorders 1997;21(8):626631. Nonalcoholic fatty liver disease has become the most typical reason for persistent liver disease and its prevalence will continue to increase as a consequence of the obesity epidemic. The actual proportion stays uncertain relying on the population studied, clinical setting, and diagnostic screening approach. While some pharmacologic brokers appear to be promising [10,11], life-style intervention (mainly diet plus exercise) remains the standard of care to keep away from disease progression [12,13]. Most research have had severe shortcomings starting from small sample measurement to brief duration [2228], or just lacking a management group [2931]. Even in strongly managed research, important variability within the dietary or train protocols make comparisons between studies and generalized conclusions difficult [32,33]. Studies have been inconsistent when assessing several types of diet (low fat, low carbohydrates, and so on) [2224,39,40], and train coaching protocols. These studies may be divided into two main sorts: those that have centered on weight reduction solely, and scientific trials that have assessed the position of a specific dietary composition on hepatic steatosis. Taken together, a 45% weight reduction by dietary intervention alone usually improves plasma aminotransferases levels and hepatic steatosis. As could be observed, independently of the kind of diet used, weight reductions starting from 6. Only a number of studies have examined the position of dietary composition along with negative caloric balance.
Comparative prices of Perindopril
#
Retailer
Average price
1
HSN
761
2
J.C. Penney
596
3
Staples
599
4
Meijer
353
5
Publix
717
6
Costco
523
7
Wendy's / Arby's Restaurants
226
8
Winn-Dixie Stores
739
9
ShopKo Stores
292
Similarly arrhythmia ekg discount perindopril 4 mg overnight delivery, pulsatile supply of glucagon in humans has greater effects in stimulating endogenous glucose manufacturing than steady infusion hypertension journal article order perindopril from india. Furthermore blood pressure normal low pulse purchase perindopril in united states online, when each insulin and glucagon are delivered intermittently and out of phase blood pressure under 60 purchase 2 mg perindopril with visa, the greater impact of glucagon in stimulating glucose production prevails over the greater impact of insulin in inhibiting this parameter [35]. This fall in malonyl-CoA brings fatty acid synthesis to a halt and causes derepression of the enzyme carnitine acyltransferase such that incoming fatty acids (made abundant by way of stimulation of lipolysis) are efficiently converted into the ketone bodies acetoacetate and 3-hydroxybutyrate. The effects of glucagon on the adipocyte markedly depend upon the species considered. Although glucagon is a potent lipolytic hormone in birds and in rodents, its results on the human adipose cell have long been disputed. Recent investigations have proven that glucagon is indeed strongly lipolytic within the human adipocyte in vitro, however that this impact is tough to demonstrate utilizing incubation of adipocytes or adipose tissue pieces as a end result of glucagon is rapidly destroyed by a proteolytic activity associated with these cells. When perifusion methods are used, the lipolytic effect of glucagon on human adipocytes can simply be demonstrated. Interestingly, within the older inhabitants the lipolytic and ketogenic, but not the hyperglycemic, responses to pulsatile glucagon are significantly lowered [37]. Other results of glucagon Other metabolic effects of glucagon embody modification of the circulatory pattern of plasma amino acids (partly because of the stimulation of gluconeogenesis), a discount in circulating ranges of cholesterol and triglycerides, and a stimulation of fibrinogen formation. Glucagon additionally stimulates insulin release, but the physiologic character of this effect is questionable [42]. Under certain circumstances, glucagon will increase renal blood circulate and glomerular filtration rate, and promotes renal loss of sodium and different ions [44]. At pharmacologic doses, glucagon stimulates adrenal catecholamine launch, an impact that has been used for the prognosis of pheochromocytoma. Combining glucagon stimulation and clonidine suppression testing has given a sensitivity of 100% and a specificity of 79% for the prognosis of pheochromocytoma [45]. Glucagon additionally exerts optimistic inotropic and chronotropic results on the center [46], effects that could be helpful, for example, in treating the cardiodepressive manifestations of poisoning by -receptor blocking agents. Glucagon and a quantity of other of its analogues, like glucagon-(1-21), which is devoid of metabolic effects, exert a potent smooth-muscle spasmolytic motion, generally used for varied diagnostic procedures or for therapeutic functions like bronchospasm [47]. Glucagon secretion is also regulated by circulating hormones and the autonomic nervous system [50,51]. The components and conditions related to inhibition of glucagon release are listed in Table 10. It has been advised that glucokinase might serve as a metabolic glucose sensor in pancreatic cells, and therefore represent a mechanism for direct regulation of glucagon launch by extracellular glucose. Intra-islet insulin, glucagon, and somatostatin release have been shown to be interrelated [52]. Using isolated perifused human islets, it has been shown that glucose generates coincident insulin and somatostatin pulses and clear antisynchronous glucagon pulses [55]. The fact that these pulses occur in isolated islets demonstrates that their origin is the islets themselves and unbiased of exterior metabolic, hormonal, or neuronal indicators. The nature of the intra-islet signal(s) coordinating the secretion of the varied endocrine cells of the islets of Langerhans is still the topic of intense investigation [5661]. Some elements of glucagon physiology and pathophysiology Glucagon as a counterregulatory hormone Numerous studies have proven that the liver is the principle website at which moment-to-moment control of glucose homeostasis takes place and that in regular humans glucagon is the most important glucose counterregulatory hormone. By antagonizing the suppressive effects of insulin on glucose manufacturing and by stimulating glucose production when appropriate, glucagon not only defends the organism in opposition to hypoglycemia, but additionally restores normoglycemia if hypoglycemia happens. Biosynthesis, secretion, and action of glucagon 141 release in some diabetic patients markedly will increase the danger of extreme hypoglycemia in these subjects. Other hormones, corresponding to epinephrine (acutely) and development hormone and cortisol (more slowly), take part within the counterregulation of the consequences of insulin, but careful clinical observations counsel that certainly glucagon is the primary line of protection against hypoglycemia [62]. Glucagon in train Glucagon levels increase progressively during prolonged train [63], throughout which blood glucose stays comparatively fixed thanks to a fine steadiness between muscle glucose uptake and liver glucose production. It occurs primarily as a end result of the -adrenergic stimulation associated with stress and undoubtedly contributes to the hyperglycemia, which is a classical finding on this condition. Glucagon in starvation Starvation is accompanied by a decline in circulating insulin and a moderate rise in plasma glucagon [65]. The major effects of glucagon during starvation are at the liver, where it contributes to the maintenance of steady liver glucose output (initially by stimulating glycogenolysis, and later by selling gluconeogenesis) and the induction of ketogenesis. Whether glucagon contributes to the stimulation of adipose tissue lipolysis during hunger continues to be disputed. Glucagon and adaptation to extrauterine life A vital rise in plasma glucagon occurs soon after start in all species investigated thus far, which suggests that glucagon has a crucial role in neonatal glucose homeostasis [66].
Gangrenous Cholecystitis Definition Gangrenous cholecystitis is a severe type of sophisticated acute cholecystitis characterised by ischemia and hemorrhagic necrosis of the gallbladder wall blood pressure youtube cheap perindopril 8 mg otc. Demographic and Clinical Features Gangrenous cholecystitis is the most common complication of acute cholecystitis blood pressure lab report purchase 2 mg perindopril fast delivery, occurring in 2% to 30% of instances blood pressure medication given during pregnancy buy 8 mg perindopril otc. It is related to higher mortality and morbidity rates than uncomplicated acute cholecystitis pulse pressure septic shock discount perindopril uk. High-risk patients are males over 50 years of age with cardiovascular disease and leukocytosis (a white blood cell count larger than 15,000/ mL). Although patients with gangrenous cholecystitis are typically more acutely unwell at presentation than those with acute cholecystitis, scientific presentation and laboratory findings may be undistinguishable from these in acute cholecystitis. Pathology Increased pressure within the gallbladder wall as a end result of marked distention of the gallbladder from cystic duct obstruction by gallstones or sludge may lead to ischemic necrosis of the gallbladder wall. Gangrene normally occurs initially within the fundus, as its vascular supply is the first to be compromised. Mucosal or intraluminal hemorrhage, ulcerations within the mucosa, and sloughed intraluminal membranes representing desquamated mucosa are findings that suggest gangrene. Focal transmural defects from perforation may be noticed on gross inspection of the gallbladder. Intraluminal membranes representing desquamative gallbladder mucosa are a specific findingthat is much less commonly noticed. Intraluminal hemorrhage is heterogeneous or echogenic materials within the gallbladder lumen or wall. Intramural and intraluminal hemorrhage is of high signal intensity on fat-suppressed T1-weighted images. Ulceration of the mucosa manifests as a hyperintense defect in the gallbladder wall on fat-suppressed T2-weighted photographs. Heterogeneous enhancement, segmental absence of enhancement, and disrupted mucosal enhancement of the gallbladder wall are extremely suggestive of gangrenous cholecystitis. Longitudinal (A) and transverse (B) ultrasound images show a sludge crammed gallbladder with intraluminal membranes (arrows) floating within the bile. There is lack of shade Doppler sign and a pericholecystic fluid collection adjoining to the disrupted wall (arrowhead). Management/Clinical Issues Urgent laparoscopic cholecystectomy must be carried out when gangrenous cholecystitis is suspected to be able to keep away from potential life-threatening problems. Conversion to open cholecystectomy is required extra usually than for noncomplicated acute cholecystitis. Intraluminal membranes, irregular or absent wall enhancement, and intramural/intraluminal hemorrhage are suggestive findings. Chronic Cholecystitis and Xanthogranulomatous Cholecystitis Chronic Cholecystitis Definition Chronic cholecystitis is a typical inflammatory situation of the gallbladder and one of the frequent forms of clinically symptomatic gallbladder disease. Demographic and Clinical Features Chronic cholecystitis happens extra typically in women than in males. Clinically patients could complain of recurrent acute right-upper-quadrant pain or intermittent biliary colic. Occasionally nonspecific symptoms corresponding to imprecise epigastric ache and nausea could be the solely criticism. Possible issues of chronic cholecystitis include repeated episodes of acute cholecystitis and gallbladder carcinoma. Rarely formation of a biliary-enteric fistula could occur, with potential subsequent gallstone ileus. Pathology Chronic cholecystitis is the result of intermittent and recurrent transient obstruction of the cystic duct or Cholecystitis 461 gallbladder neck by stones. Episodes of obstruction cause low-grade irritation and subsequent fibrosis of the gallbladder wall. As a consequence, irregular thickening of the gallbladder wall develops and the gallbladder could become small, contracted, and adherent to the adjoining organs and omentum.
Structure of the insulin molecule the first construction A- and B-chain of insulin itself has been recognized for close to arrhythmia lying down discount perindopril 50 years [88] high blood pressure medication valsartan perindopril 4mg for sale. The N-terminal signal peptide (24 amino acids) is cleaved cotranslationally to yield proinsulin blood pressure medication zanidip cheap perindopril. Proinsulin to insulin conversion occurs by cleavage at two dibasic amino acids sequences by the B-chain/C-peptide and C-peptide/A-chain junctions to launch the C-peptide moiety yielding the insulin molecule with the 2 independent disulphide-linked A- and B-chains accurately aligned [88] blood pressure journal pdf cheap perindopril american express. Proinsulin biosynthesis: effectors and stimulus-response coupling mechanisms Proinsulin biosynthesis is translationally controlled by sure nutrients, neurotransmitters, and hormones, however glucose is essentially the most physiologically related [91]. Significant glucose-induced proinsulin biosynthesis may be noticed after a 2030-min lag period that reaches a most fee (2030-fold increase above basal) by 60 min [91]. Of the peptide hormones that stimulate Relevance to human type 2 diabetes Recent research in human islets assist the notion that faulty insulin gene expression might play a task in human sort 2 diabetes. Insulin biosynthesis Introduction the earlier part outlines that insulin gene transcription is a extremely controlled course of. The signal peptide + insulin + C-peptide moieties comprise preproinsulin, and the insulin + C-peptide moieties comprise proinsulin. Epinepherine can be worthy of point out for particularly inhibiting glucose-induced proinsulin biosynthesis because it does glucose-induced insulin secretion [91]. Unlike that for glucose-induced insulin secretion, the secondary indicators that lead to a rise in proinsulin biosynthesis are much less properly defined. Glucose metabolism is required for glucose-induction of each proinsulin biosynthesis and insulin secretion, however several strains of evidence indicate that the stimulus-response coupling mechanism for these -cell functions are fairly distinct [91,92]. Somatostatin is a potent inhibitor of insulin secretion, but has no impact on proinsulin biosynthesis [91,92]. Long-chain fatty acids, when applied acutely, are marked potentiators of glucose-induced insulin secretion, but if something modestly inhibit glucose-induced proinsulin biosynthesis [91,92]. Proinsulin biosynthesis: translational control mechanism Glucose modestly will increase basic protein synthesis within the cell 1. However, the effect of glucose on proinsulin synthesis translation is much higher, and might reach 10-fold stimulation above basal [91,92]. This signifies a particular effect of glucose on translational management of proinsulin biosynthesis. It must be famous that proinsulin is simply one of a small subset of -cell proteins (50 in all) [92] whose biosynthesis is regulated by glucose at the translational degree. Generally, analogous to other neuroendocrine cells, the process of -granule biogenesis also needs to require different factors including intraluminal acidic pH 6. Maturation of granules entails proinsulin conversion, progressive intragranular acidification, loss of the clathrin-coated regions, and formation of hexameric insulin crystals [91,93]. This is according to the presence of the des 31,32 proinsulin conversion intermediates in the human circulation but negligible ranges of des sixty four,sixty five proinsulin [91]. The left panel indicates the intracellular compartments by which proinsulin is sequentially transported via, and the right panel indicates the kinetics of the preproinsulin biosynthetic/processing/secretory process in these compartments. This generates an advanced phenotype of multiple endocrine disorders as a result of common abnormal prohormone processing, certainly one of which could be very low insulin levels and high proinsulin ranges, along with abnormal glucose homeostasis, according to faulty proinsulin processing [88]. There are two potential pathways of proteolytic conversion of proinsulin to insulin. In human cells, the route by way of des 31,32 proinsulin predominates as illustrated by the bigger measurement of this pathway. Fortunately, the granule contains an intraorganellar surroundings of 110 mM free Ca2+ and acidic pH 5. Thus, plainly proinsulin conversion is adaptable to changes in glucose by coordinate regulation of the endopeptidases that catalyze processing [91,92]. It should be famous that under regular circumstances, the storage compartment of insulin in mature granules far exceeds the compartment undergoing transport/exocytosis, so that in a 1-h stimulation by glucose only 12% of the insulin content material of a main islet cell is secreted [92]. The insulin content of a cell is kept at a relatively constant level beneath regular physiologic conditions the place secreted insulin is rapidly changed on the biosynthetic degree. It is feasible that genetic defects in the proinsulin conversion enzyme genes or the insulin gene itself hamper proinsulin conversion, resulting in an elevated proportion of proinsulin secreted. However, such genetic mutations are very rare, yet hyperproinsulinemia is a standard trait of type 2 diabetes [91].
Order cheap perindopril on-line. Care Touch | Wrist Blood Pressure Monitor | Fully Automatic | Platinum Series | Review and Demo.
On the other hand hypertension goals generic perindopril 2 mg with visa, age blood pressure medication african american purchase perindopril paypal, gender hypertension used in a sentence buy perindopril 2 mg visa, distribution of physique fat prehypertension to treat or not to treat generic 4 mg perindopril with mastercard, food regimen, and menstrual section are general physiologic covariates of insulin sensitivity. Evidence obtained in Pima Indians [67] demonstrates that genetic elements are at work in the distribution of insulin sensitivity in the population. Thus, glucose oxidation is extra delicate (lower obvious half-maximum) however saturates earlier (lower maximum) than glycogen synthesis; the latter behaves as a pathway with low sensitivity and excessive capacity. Skeletal muscle is the predominant web site of insulin-mediated net glycogen synthesis; insulin additionally has a potent effect to increase hepatic glycogen synthesis though its contribution to whole body glycogen synthesis is small compared to skeletal muscle. The increment in carbohydrate oxidation that follows systemic insulin administration happens in muscle as well as other tissues together with liver and adipocytes. The reciprocal sample of modifications of glucose disposal/oxidation on the one hand, and lipid oxidation/utilization on the other, introduces the concept of substrate competition [70,71]. This impact is reinforced by the glucose-induced rise in insulin, which additional reduces the provision of lipid substrates by instantly inhibiting lipolysis. The extent to which insulin action in target tissues is direct somewhat than mediated by shifts in substrate supply may be appreciated by evaluating systemic with local insulin administration. Under these situations, insulin stimulates forearm glucose uptake and lactate launch, but induces only minimal modifications in the local respiratory quotient (0. This indicates that the forearm tissues proceed to rely mostly on lipid oxidation for vitality production, and that the vast majority of insulin-stimulated glucose uptake is channeled to glycogen [55]. In contrast, when comparable hyperinsulinemia is created by systemic insulin administration (with maintenance of euglycemia), the leg respiratory quotient increases from zero. Increased amino acid provision enhances glucose production under conditions of insulin deficiency or resistance, and limits glucose utilization within the insulinized state [60]. In summary, each of the three main substrates, if current in extreme quantities (whether by endogenous manufacturing or exogenous administration), can decrease the level of the other two by stimulating insulin release. In this capability, glucose is clearly favored, being a means more potent secretagogue than fat or amino acids. Insulin actions in vivo: glucose metabolism 225 Cellular, biochemical, and molecular mechanisms of insulin action (see additionally Chapter 12) Insulin receptor/insulin receptor tyrosine kinase the insulin receptor is a glycoprotein consisting of two subunits and two subunits linked by disulfide bonds and expresses insulin-stimulated kinase activity directed towards its personal tyrosine residues [12,8487]. Insulin receptor phosphorylation of the subunit, with subsequent activation of insulin receptor tyrosine kinase, represents step one in the motion of insulin on glucose metabolism. Insulin receptors devoid of tyrosine exercise are completely ineffective in mediating insulin stimulation of cellular metabolism. Mutagenesis of any of the three main phosphorylation websites (at residue 1158, 1163, and 1162) impairs the insulin receptor kinase activity, and this is related to a marked decreased within the acute metabolic and growth-promoting results of insulin [12,8688]. This decreases glycogen synthase phosphorylation, resulting in activation of the enzyme. Glucose transport Activation of the insulin sign transduction system in insulin target tissues leads to the stimulation of glucose transport. It is positioned primarily in the plasma membrane, the place its focus changes little after the addition of insulin. It has a low Km (1 mmol L-1) and is nicely fitted to its perform, which is to mediate basal glucose uptake. In response to physiologic euglycemic Insulin actions in vivo: glucose metabolism 227 Table 14. In the low physiologic vary of hyperinsulinemia, glycogen synthesis and glucose oxidation are of roughly equal quantitative importance. With rising plasma insulin concentrations, glycogen synthesis becomes predominant [63,68]. Glycogen synthase is the important thing insulinregulated enzyme that controls the speed of muscle glycogen formation [100102]. The impact of insulin on glycogen synthase gene transcription and translation in vivo has been studied by using the euglycemic insulin clamp in combination with muscle biopsies. Rather, insulin converts the inactive (phosphorylated) form of glycogen synthase to the lively (dephosphorylated) form of the enzyme [5658]. Glycolysis/glucose oxidation Glucose oxidation accounts for roughly 90% of total glycolytic flux, while anaerobic glycolysis accounts for the genase. Oral glucose At any point in time, the glycemic response to exogenous glucose is the stability between the speed at which glucose seems within the systemic circulation (from oral as nicely as endogenous sources) and the speed at which glucose is disposed of.