Order fertomid 50mg without prescriptionOperative photograph taken following removal of a large axillary tumor exhibits all the muscular tissues of the axillary area women's health clinic university of maryland fertomid 50mg with amex, the axillary sheath women's health clinic utica ny cheap fertomid 50mg line, and corresponding cords of the brachial plexus women's health center west bloomfield buy discount fertomid 50mg on line. Neurologic exploration Identify the sheath of the brachial plexus and axillary vessels underneath the indifferent conjoint tendon womens health 5 minute workout purchase 50 mg fertomid overnight delivery. The musculocutaneous nerve comes across the decrease border of the coracoid under the pectoralis minor muscle. The axillary nerve comes off deeper from the posterior wire and travels toward the shoulder joint. Vascular exploration Completely exposure and control the axillary vessels and brachial plexus proximally by opening the pedicle sheath and placing loops around the major buildings; careful dissection is then used to mobilize these constructions distally into the arm. Mobilization often is critical to facilitate adequate publicity prior to tumor resection. Resection of tumor All of the feeding branches coming into into the mass are serially ligated and transected. The tumor is removed, tagged for orientation, and despatched to pathology for margins and histologic analysis. Lymphatic involvement, incessantly seen in sufferers with breast cancer extending into the axilla, requires meticulous dissection of the axillary and subclavian vessels proximally; sampling of lymph nodes is crucial in patient with carcinomas or melanoma. Resection of Posterior Axillary Tumors Resection of Anterior Axillary and Chest Wall Tumors Tumors involving the pectoralis and serratus anterior may be resected safely following identification and mobilization of the crucial neurovascular buildings; these muscles could also be elevated directly off the underlying chest wall. Resection of high-grade sarcomas could require sacrifice of a quantity of main branches of the brachial plexus to obtain an adequate oncologic margin. Chest wall involvement requires thoracotomy and resection of contiguous ribs; the underlying lung is deflated before opening the chest cavity to protect it. Intrathoracic extent of tumor is determined by palpation of the pleural surface following thoracotomy; osteotomy of the ribs using a rib cutter beneath direct visualization permits en bloc removing of the involved chest wall. Identify the latissimus insertion into the humerus, which defines the posterior facet of the axilla distal and posterior to the pectoralis insertion. Before performing tendon launch, determine and protect the axillary nerve proximal to and the radial nerve distal to the tendon; both nerves serve to tether the brachial plexus and reduce the ability to retract the plexus. Tumor involvement of the latissimus could require sacrifice of one or each of those nerves. The latissimus muscle may be elevated off the chest wall as needed for tumor resection. Chest wall involvement might require thoracotomy and resection of contiguous ribs; deflate the lung before opening the chest cavity to defend the underlying lung. Intrathoracic extent of tumor could additionally be determined by palpation of the pleural surface following thoracotomy. Osteotomy of the ribs using a rib cutter underneath direct visualization permits en bloc removing of the concerned chest wall. Reconstruction Following Tumor Resection Repair and reconstruction of the axilla is critical following tumor resection. Insertion of an epineural catheter into the sheath of the brachial plexus permits postoperative administration of local anesthetics similar to bupivacaine (Marcaine) to reduce postoperative ache. Extremely giant, low-grade, fibrosarcoma of the axilla extending from the thoracic outlet to the posterior axillary line and to the level of the breast. All tissues have been removed through a combination of the anterior and posterior parts of the utilitarian shoulder girdle incision. Intraoperative photograph taken before reconstruction and reattachment of the muscular tissues of the again and anterior pectoralis major. This photograph demonstrates the benefit of a transpectoralis method anteriorly combined with a posterior approach. Reattachment of the conjoint tendon and pectoralis minor to the coracoid with the usage of mattressed, nonabsorbable sutures covers the brachial plexus and axillary vessels. Defects of the chest wall can be coated with local rotation flaps using the latissimus dorsi or pectoralis main muscle, which may be tenodesed to the subscapularis tendon as wanted. Careful wound closure over closed suction drains and placement of absorptive padding within the axilla reduce the chance of pores and skin maceration and wound infection.
Cheap fertomid 50mg on-lineThicker tendons can assist a two- or four-strand greedy restore with a 2-0 pregnancy 7 weeks 1 day quality fertomid 50 mg, 3-0 menopause journal order generic fertomid, or 4-0 nonabsorbable braided suture (eg pregnancy induced hypertension buy generic fertomid line, Ethibond breast cancer oakley sunglasses buy 50mg fertomid free shipping, Ticron, or Fiberwire), optionally reinforced with a 5-0 or 6-0 monofilament epitendinous suture positioned in a easy running or cross-stitch fashion. In general, restore power is related to number of suture strands crossing the repair website, the thickness of the suture, and the locking type of the stitch. The strongest repairs are the Silfverski�ld cross-stitch for flat tendons, and the four-strand cruciate suture for tendons capable of settle for a core suture. Silfverski�ld cross-stitch (which can be used as a circumferential epitendinous tidying suture over a core suture). A figure eight or running cross-stitch with a 5-0 nonabsorbable suture could be positioned within the tendon, taking care to keep away from shortening the tendon. The suture can be removed in 2 to three weeks, but the splinting ought to proceed for a complete of 6 weeks full time and another 6 weeks at night time. The suture (passing from left to right in A) goes by way of the skin and tendon proximally and distally. Extend and scale back the distal phalanx, bringing it up to the fragment, and stabilizing it by advancing the 0. Dorsal pins buttress the fragment, and the longitudinal pin reduces the flexion and subluxation. Repair the lateral band or bands with single 4-0 or 5-0 monofilament suture in a figure eight fashion. Consider V-Y development of the central tendon or a "turndown" of the central slip proximal to the laceration to cowl the defect. Disrupt the unfastened alveolar tissue between the tendon and periosteum as little as potential. Note how difficult it will be for a laceration to reduce all the way across the extensor mechanism. This example has been repaired with a running, cross-stitch suture (Silfverski�ld). Results are often less than good, particularly in cases with tendon loss, the place some loss of movement ought to be expected. The distal locking sew is positioned on one aspect of the tendon however not pulled tight till the tendon ends are accurately approximated. Use a 3-0 or 4-0 braided nonabsorbable suture, reinforced with a circumferential running cross-stitch 5-0 or 6-0 monofilament suture. The extensor retinaculum is incised for repair and retrieval of the proximal tendon stump. Retinacular closure is performed with a 4-0 absorbable suture to stop tendon bowstringing. A portion of the retinaculum could must be excised to allow the restore site to glide easily. Make a generous incision to decide the resting orientation of the tendons earlier than d�bridement and restore. It could additionally be useful to tag proximal tendon ends with labels to outline them earlier than further dissection changes their position. Tetanus immune globulin should be given for tetanus-prone wounds in sufferers with unknown or incomplete vaccination historical past. The biggest safety against tetanus is a completed childhood vaccination sequence. Side-to-side restore to adjacent extensor tendons or use of a free tendon graft is occasionally wanted for therapy of persistent accidents involving different tendons. Digital extensor mechanism is very delicate to shortening, with ensuing loss of flexion. Before exploring proximal harm, locate and label individual tendon ends (based on location). Associated nerve harm (especially the posterior interosseous nerve) can make diagnosis and remedy tough. Suture strategies To most easily do the Silfverski�ld cross-stitch, start on the aspect of the tendon closest to the surgeon. After the first knot is tied, advance away across the tendon, maintaining the needle pointed back on the surgeon for the horizontal element of the stitch.
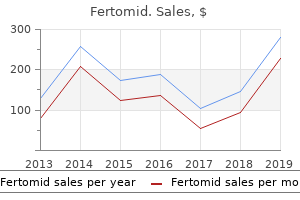
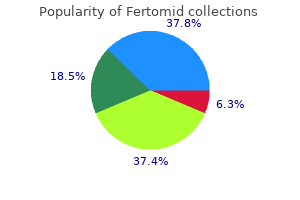
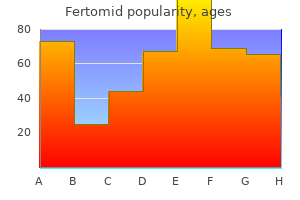
| Comparative prices of Fertomid | | # | Retailer | Average price | | 1 | Abercrombie & Fitch | 396 | | 2 | Staples | 175 | | 3 | Raley's | 983 | | 4 | Ross Stores | 899 | | 5 | Meijer | 132 | | 6 | AutoZone | 252 | | 7 | Darden Restaurants | 808 | | 8 | Starbucks | 197 | | 9 | IKEA North America | 450 |
Discount fertomid 50mg on-lineResults of early custom prostheses have been disappointing menstruation joke generic fertomid 50 mg visa, leading many surgeons to use allografts or other methods of reconstruction menopause night sweats buy discount fertomid 50 mg on-line. More just lately pregnancy kit cost generic 50mg fertomid fast delivery, there was elevated curiosity in endoprosthetic reconstruction as multiple facilities have reported improved outcomes women's health center macomb il discount fertomid generic. Informal polling of members of the Musculoskeletal Tumor Society has shown a major swing from a majority of members using primarily allograft reconstructions to a majority of members using endoprosthetic reconstruction. Recently published results looking at long-term survival of 242 cemented endoprosthetic replacements9 demonstrated an general survival of 88% at 5 years and 85% at 10 years (Table 1). Prosthetic survival diversified by sort and placement, with the poorest survival seen in patients with early customdesigned implants and in sufferers with proximal tibial replacements. Outcomes following reconstruction of the distal femur in a hundred and ten patients had been judged pretty much as good to wonderful in 85% of sufferers. Most sufferers have depressed immune systems from chronic disease, chemotherapy, and malnutrition. Patients usually are anemic and have clotting abnormalities, together with thrombocytopenia. The anatomic location of a tumor and essential resection could lead to vital disruption of the venous and lymphatic drainage of the extremity during resection, resulting in venous stasis, swelling, and lymphedema. This can lead quickly to flap necrosis through the postoperative interval, secondary an infection, and eventual amputation. Finally, oncologic complications, together with native recurrence of tumor or tissue necrosis from radiation, might end in failure of a limb-sparing procedure. Complications specific to endoprosthetic reconstruction could also be associated to mechanical or biologic elements. Prosthetic fracture, disassociation of modular components, fatigue failure, and polyethylene put on have been described. Improved implant designs, metallurgy, and manufacturing methods can reduce the incidence of those problems considerably. Biologic failure of an endoprosthesis could occur on account of joint instability, aseptic loosening, or periprosthetic fracture of bone around the prosthesis. Meticulous attention to gentle tissue reconstruction has nearly eliminated joint instability as an issue. The use of circumferential porous coating, correctly sized large-diameter stems, and third-generation cementation methods has helped to forestall aseptic loosening in our patients. Surgical method and the utilization of polished cemented stems have prevented periprosthetic fractures throughout surgical procedure. Several sufferers with secondary, late fractures as a result of blunt trauma (eg, falls, auto accidents) have been treated efficiently with casting and protected weight bearing. Its success also has expanded the indications to embody bone defects for non-oncologic issues. Kaplan-Meier survival curve evaluating all Modular Replacement Systems by anatomic site. Proximal femur and proximal humerus replacements have essentially the most superior survival results, adopted by distal femur, after which proximal tibia. Kaplan-Meier survival curve showing superior outcomes of modular replacement system when compared to customized prostheses over all anatomic sites. Today, extra endoprosthetic reconstructions are performed for non-oncologic reconstructions than for osteosarcomas. Ongoing research frequently strives to improve the end result following endoprosthetic reconstruction. Continued work on improved metallurgy and polymers, particularly with the introduction of cross-linked polyethylene, promises improved long-term durability. Routine use of premixed antibiotic cement and experimentation with antimicrobial implant surfaces might help to scale back the danger of periprosthetic infection. New strategies for tendon attachment to the prosthesis embody novel clamps and ingrowth surfaces to promote improved junctional power. New implant technologies such because the Rephyisis noninvasive expandable prosthesis provide hope to younger children with few various choices. New fixation methods, including hydroxyapatite stems with porous coated surfaces, may be of nice value in non-oncologic sufferers.
Generic fertomid 50mg free shippingA warm breast cancer 2020 order discount fertomid, moist wrap can be utilized around the wrist to present further stretching of the wrist earlier than actions women's health clinic winnipeg buy fertomid 50mg amex. Examples of exercises: Pronation and supination: Stretching could be achieved by holding a hammer or frying pan as a weight in the course of the motions women's health clinic brisbane northside order 50 mg fertomid with mastercard. Additionally women's health clinic north vancouver purchase discount fertomid line, the nerve will be passing immediately over an area of soppy tissue closure and may be affected by the encompassing scar tissue. Other potential problems might happen as a result of the Kirschner wire, corresponding to migration, an infection, and nerve injury. Partial excision of the triangular fibrocartilage complicated articular disk: a biomechanical study. Proceedings of the Annual Meeting of the American Society for Surgery of the Hand, Sept. Ulnotriquetral augmentation tenodesis: a reconstructive process for dorsal subluxation of the distal radioulnar joint. Studies on the tendinous compartments of the extensor muscular tissues on the back of the human hand and their tendon sheaths. Hui-Linscheid reconstruction Successful short-term scientific outcomes have been reported in a small patient series by Hui and Linscheid, with sufferers reporting passable and excellent outcomes. Pain and dysesthesias at dorsal branch of ulnar nerve: Care should be taken when inserting sutures for imbrication of the extensor retinaculum to keep away from injury to surrounding tissues or nerve buildings. Damage to the ulnar nerve through the surgical procedure is concerning due to its anatomic location. The nerve is immediately exposed after the opening incision and is susceptible Chapter fifty two Arthroscopic Dorsal Radiocarpal Ligament Repair David J. They are finest seen by way of a volar radial portal and are amenable to arthroscopic repair. The capsular ligaments, together with the radioscaphocapitate, radiolunotriquetral, ulnolunate, ulnotriquetral, dorsal radiocarpal, and dorsal intercarpal ligaments, can be considered secondary stabilizers. It originates on the tubercle of Lister and strikes obliquely in a distal and ulnar path to connect to the tubercle of the triquetrum. It can differ its size by altering the angle between the 2 arms while maintaining its stabilizing effect on the scapholunate joint throughout wrist flexion and extension. Of this subgroup one patient had Geissler stage 2 instability and one had a Geissler stage 3 or four tear. If midcarpal instability is present, the affected person could have a positive midcarpal shift check. In nondissociative carpal instability, the pain is believed to be attributable to dynamic joint incongruity. Failure to reply is a sign for a radiocarpal cortisone injection followed by 1 further month of splinting. Patients who continue to have wrist ache ought to then bear imaging studies to rule out related intracarpal pathology. Positioning the patient is positioned supine on the operating table with the arm abducted. This could embody traction from the overhead lights or a shoulder holder together with 5- to 10-lb sand luggage attached to an arm sling. A fiberoptic mild source, video monitor, and printer are also normal tools. A variety of curved and straight 18-gauge spinal needles are used for passage of an absorbable 2-0 suture for the outside-in repair. The normal dorsal portals are established, including the 3-4 and 4-5 portals, a midcarpal radial portal, and a midcarpal ulnar portal. Be certain to assess the scapholunate and lunotriquetral intervals from the midcarpal joint to assess any dynamic instability. When performing capsular shrinkage, use copious irrigation to stop thermal chondral injury. At the primary postoperative visit the sutures are eliminated and the patient is placed in a below-elbow cast for a complete immobilization time of 6 weeks. Wrist movement with use of a removable splint for comfort is instituted after solid elimination. A dorsal capsulodesis was performed within the seven sufferers with scapholunate instability.
Generic fertomid 50mg with visaThe correct ulnar and radial collateral ligaments originate from fossae of the condyle of the metacarpal head on the radial and ulnar sides and move obliquely from dorsal proximal to volar distal to insert on the volar third of the bottom of the proximal phalanx womens health usa 2012-06pdf buy fertomid 50 mg visa. The ligament widens because it goes from its metacarpal origin to its proximal phalangeal insertion breast cancer diet buy fertomid 50 mg mastercard. By definition menopause hot flashes icd 9 generic fertomid 50mg line, to have a whole ligament rupture women's health center fort wayne generic fertomid 50 mg with visa, both the proper and the accent collateral ligaments should be torn. The ligament tears distally at or near its insertion on the volar ulnar base of the proximal phalanx. Hence, the avulsed ligament is separated from its deep insertion by the aponeurosis, preventing ligament healing. Most generally, chronic laxity is because of lack of recognition of the pathology and subsequently insufficient or late therapy. Patients are questioned about pain in the thumb, particularly if it is exacerbated by forceful pinch and grasp and torsional activities like turning keys in locks, turning doorknobs, or unscrewing jar tops. The joint may be angulated or rotated in its resting posture if the collateral ligament is grossly incompetent and the instability is chronic. Palpation of a fullness or soft tissue mass on the ulnar facet of the metacarpal head is strongly suggestive of a Stener lesion. Laxity in extension suggests that the accent and correct collateral ligaments are each torn. A more subtle, however usually more useful, finding is the presence or absence of a discrete endpoint to joint opening when careworn. An isolated tear of the dorsal joint capsule very rarely causes volar subluxation without an associated collateral ligament damage. A comparison lateral radiograph of the contralateral thumb is extraordinarily useful if volar subluxation is suspected. Most experienced clinicians rely almost completely on physical examination and static plain radiographs to make the diagnosis. Theoretically, the asymmetric put on of the articular cartilage ensuing from chronic laxity causes degeneration of the articular cartilage. The extra chronic the harm and the extra dramatic the laxity and deformity, the extra doubtless the need for substitute of the ligament with a graft. Positioning the patient is supine on the operating room table with the arm on a hand desk at an angle barely less than perpendicular to the torso. Preoperative Planning the patient is asked to actively bring all 5 digits collectively and concurrently flex the wrist in opposition to resistance. A chevron-shaped incision is made centered over the ulnar facet of the metacarpophalangeal joint. The adductor aponeurosis is incised longitudinally about 2 mm from the extensor expansion, offering a cuff of tissue dorsally to facilitate an adequate repair at the finish of the process. Excision of the ulnar collateral ligament remnants exposes the metacarpophalangeal joint, the metacarpal head, and the bottom of the proximal phalanx. The diameter of the hole required is decided by the scale of the tendon graft to be used for reconstruction. The preferred donor is the palmaris longus, which is often pretty skinny and might fit in a relatively small hole. Make the holes at an angle of about 45 degrees to the bone surface and direct them toward each other to be able to converge throughout the medullary canal and create a bone tunnel. Prebend a 28-gauge stainless steel wire into the approximate arc of curvature of the bone tunnel to facilitate its passage. Most often the small, medium, and huge gouges are used to create one large gap since each ends of the tendon graft are passed via this hole. The adductor aponeurosis has been divided and the collateral ligament remnants have been excised. The tendon is pulled utilizing moderately firm traction and a circular movement of the wire. Avoid fracturing the bony bridge between the gouge holes by pulling too firmly on the wire with a vector of pull away from the bone. Remove this wire and tie the ulnar finish of the wire beforehand positioned in the metacarpal bone tunnel round both ends of the tendon graft. Suture the knot to the adjoining periosteum with two mattress sutures stitches of 3-0 braided artificial suture. Alternatively, place a bone anchor adjacent to the metacarpal tunnel on the radial aspect and use the loaded sutures to secure the knot.
Syndromes - Healthy fats
- People who follow a vegetarian or vegan diet should try to eat vitamin B12-fortified foods or talk to their doctor about taking B12 supplements.
- Eating disorders
- A needle is gently inserted into the vein.
- This is the first time the person has had a seizure.
- Pale appearance (pallor) with cold skin
- What other symptoms came before or with the abnormal posturing?
- Rapid brain development occurs.
50mg fertomid amexPatients who undergo amputation proximal to the insertions of the deltoid and pectoralis major muscles have far higher difficulties adjusting to their prosthesis than do those that have undergone a extra distal amputation women's health clinic uihc order fertomid 50mg fast delivery. Below-elbow amputations ought to protect the maximal length of both radius and ulna menstruation relief discount fertomid online. Although tumors of the hand are treated by a regular below-elbow amputation pregnancy symptoms at 4 weeks purchase fertomid 50mg, performed via the distal third of the forearm womens health nyc purchase fertomid cheap, tumors of the distal forearm require the next amputation and warrant particular consideration. Additional length in a really quick stump can be obtained by releasing the biceps tendon; enough flexion of the stump shall be provided by the brachialis muscle. Local recurrence formerly was considered a main indication for amputation, however the mere presence of a recurrent sarcoma not is an instantaneous indication for an amputation. Major vascular involvement the neurovascular bundle throughout the arm is tightly integrated in a closed anatomic space. The cephalic vein usually provides adequate collateral move if the brachial or the axillary vein has to be sacrificed. However, though the tumor mass often could be delicately dissected off the brachial artery, generally of vascular involvement the brachial artery is extensively encased and amputation is inevitable. The compact nature of the vascular provide to the wrist makes involvement of the radial and ulnar arteries likely when a large tumor invades the volar aspect of the distal forearm. In such a case, the incidence of morbidity and failure related to resection and reconstruction using a vascular graft of considered one of these vessels is prohibitively excessive. Major nerve involvement In common, one nerve across the arm may be sacrificed, and a two-nerve deficit is tolerated. Complete staging allows dedication of full tumor extent and, as a result, the positioning for skin incision, form of the flaps, and web site of osteotomy. In common, the extra proximal of the two ranges of involvement (ie, bone or gentle tissue) determines the extent of amputation. Above-elbow amputations are carried out for superior soft tissue and bone sarcomas of the forearm. Skin incisions and osteotomy sites for metaphyseal (high), diaphyseal, and supracondylar above-elbow amputations. Below-elbow amputations are carried out for superior soft tissue and bone tumors of the forearm and hand. Clinical photograph (C) and plain radiograph (D) displaying high-grade sarcoma of the first metacarpus, requiring below-elbow amputation to obtain local tumor control. The recurrent illness is subtle, and broad resection would lead to loss of neurovascular structures and all flexor tendons, and would end with an in depth gentle tissue defect in a beforehand irradiated surgical area. Below-elbow amputation was carried out, subsequently following the beforehand deliberate incision (outlined). However, medial�lateral flaps often could also be wanted because of native tumor anatomy. They are pulled roughly 2 cm from their muscular bed, doubly ligated with nonabsorbable monofilament suture, and minimize with a knife. Myodesis is reinforced by Dacron tapes, passed by way of drill-holes made in the reduce end of the bone. Osteotomies are performed at the applicable location, as decided by the preoperative imaging research. An epineural catheter, which provides continuous circulate of local analgesics (specifically zero. Stump edema hardly ever is a significant drawback within the higher extremity, and prosthesis coaching should begin as soon as potential after surgical procedure. Active and passive range-of-motion exercises across the shoulder and elbow (if it exists) are practiced as tolerated. These approaches have clear disadvantages, nevertheless, together with excessive danger of tumor cell contamination to the encircling buildings and residual tumor tissue at the site as a result of issue in demarcating tumor from healthy tissue. These contribute to incomplete resection of the tumor in addition to excessive local recurrence charges of the spinal malignant tumor. Type 1 or 2 still could be a candidate for radiation remedy, chemotherapy, corpectomy, or hemivertebrectomy. This embolization method dramatically reduces intraoperative bleeding without compromising spinal twine function. Surgical indication for metastatic tumors Surgical strategy for spinal metastases (Table 2) consists of three prognostic elements: (1) grade of malignancy; (2) visceral metastases; and (3) bone metastases. Currently, a thoracoscopic or mini-open strategy is most well-liked for anterior dissection.
Purchase cheapest fertomidBefore cementing pregnancy 7dpo 50mg fertomid sale, 100 mg of hydrocortisone (SoluCortef) is given intravenously to defend towards fats embolism women's health quick workout cheap fertomid 50mg on-line. The deleterious effects of a fats embolism are as a end result of menstrual symptoms but no period discount 50mg fertomid with visa a massive inflammatory response in the lungs menstruation 35 day cycle best purchase fertomid. Once anesthesia is administered, the urinary catheter is positioned, and the vancomycin and gentamicin are administered, the affected person is rolled to the lateral decubitus position, with all stress points rigorously protected. A longitudinal lateral incision is produced from the tibial tubercle to as far proximal as needed. It can be ex- tended to the tip of the trochanter and then on to the anterior superior iliac backbone if a complete femur endoprosthesis is deliberate. The lateral intermuscular septum is recognized and the complete vastus lateralis may be launched from its posterolateral insertion after tying all the perforators before cutting them. Then the complete vastus lateralis can be flipped up over the femur, exposing the complete length of the bone. Because the tibial tubercle is a considerably laterally positioned structure, care must be taken to avoid avulsion of the patellar tendon. Because a few of the blood supply to the pores and skin and subcutaneous tissue is inevitably compromised through the development of the flaps and since all the geniculate vessels are routinely ligated as part of the resection of the distal femur, the risk for ischemic flap necrosis is increased. Surgical method utilizing the newly described anterior (transadductor) strategy to the distal femur. The vastus medialis remains connected to the overlying pores and skin, primarily forming a myocutaneous flap. The termination of the sartorial canal containing the superficial femoral artery and vein is dissected free. The remaining attachment of the adductor magnus tendon to the distal femur is released. Relationship of the superficial femoral artery to the popliteal area and the adductor magnus tendon. In addition, a proper sartorius muscle switch could be performed by way of this incision to recreate or to substitute either partial or complete vastus medialis loss. The vastus medialis has remained hooked up to the overlying skin, thus emphasizing the aim of this approach. If a lateral interlocking hip nail is required, a separate proximal, lateral, normal hip-like incision is made. If gentle tissue closure is taken into account to be an issue, this approach is recommended. This permits for a medial gastrocnemius flap by merely extending the incision distally. The medial gastrocnemius muscle is at all times most well-liked to a lateral gastrocnemius muscle because the medial gastrocnemius muscle is bigger and longer than the lateral gastrocnemius muscle. It permits a larger area to be coated, both longitudinally and transversely throughout the prosthesis and knee joint, respectively. Skin flap necrosis, wound dehiscence, hemarthrosis, effusions, and different wound problems are uncommon (1% to 5%). If vascular resection and reconstruction are preoperative prospects, the superficial femoral and popliteal vessels are immediately exposed. With the patient within the supine position and the surgeon standing on the medial aspect of the knee (opposite facet of the table), a long, medial paramedian skin incision is made. The incision extends proximally alongside the junction of the rectus femoris and vastus medialis muscular tissues and curves distally across the medial border of the patella to the level of the pes anserinus. Proximal Interval and Creation of Musculocutaneous Flap the interval between the rectus femoris and vastus medialis muscle tissue is recognized and opened to expose the underlying vastus intermedius muscle. It is important not to separate the overlying muscle from its fasciocutaneous coverage, which might defeat the aim of this approach. Exposure of Intermuscular Septum and Adductor Hiatus the aircraft between the vastus medialis and the medial femoral condyle is identified distally (similar to the subvastus approach). The vastus medialis muscle is dissected off the medial femoral condyle in an extra-articular style and retracted medially, away from the knee capsule. By sweeping the fibers of the muscle from the intermuscular septum with a sponge, the intermuscular septum, the adductor hiatus, and the adductor magnus tendon are uncovered.
Buy fertomid on line amexAchieve hemostasis and shut the capsule pregnancy 7 weeks spotting buy fertomid toronto, retinaculum zinc menstrual cramps buy 50 mg fertomid visa, and skin in the manner described earlier pregnancy 8 weeks 1 day buy fertomid 50mg cheap. If this trial discount reveals that the proximal hamate is outstanding in the midcarpal joint or the hamate�lunate articulation is incongruous contemporary women's health issues for today and the future 5th edition pdf generic 50 mg fertomid otc, carry out a hamate osteotomy in the identical method and at the similar stage as the capitate osteotomy. Osteotomy Fixation Compress the two cut surfaces of the capitate manually as mentioned earlier in preparation for placement of a cannulated, headless compression screw. The capitate osteotomy is carried out at the waist, which corresponds to the extent of the scaphotrapeziotrapezoidal joints. Posteroanterior radiograph after vascularized bone grafting and capitate shortening osteotomy. Examine the cartilage shell of the lunate earlier than harvesting the vascularized graft. Elevate the vascular pedicle with its perivascular tissue sufficiently to enable tension-free placement of the graft. Remove the forged four to 5 weeks after surgical procedure and initiate supervised therapy emphasizing energetic wrist motion. Over the following 4 weeks the patient can progress to active assisted and then passive range-of-motion workouts. Patients present process revascularization of the lunate are followed for 1 to 3 years. Grip strength was improved by 25%, in the end measuring 60% to 100% of the alternative side. Seventy-seven p.c of patients confirmed no additional collapse on postsurgical radiographs. Waitayawinyu et al9 described the results of 14 patients who had capitate shortening osteotomy with vascularized bone grafting for Kienb�ck illness; all had constructive ulna variance. Continued irritation or disease development may cause persistent pain, which may require temporary periods of splinting throughout symptomatic flares. Vascularized bone graft from the iliac crest for the treatment of nonunion of the proximal part of the scaphoid with an avascular fragment. Chapter 25 Ligament Stabilization of the Unstable Thumb Carpometacarpal Joint Richard Y. Of these, the dorsoradial and volar beak ligaments are an important in preventing dorsoradial subluxation of the thumb metacarpal. This maneuver will subluxate the thumb metacarpal base radially, thereby demonstrating the degree of laxity within the radial direction. Therefore, it is important to elicit from the affected person the exact signs and their severity. Pinch energy and opposition must be examined and compared to the contralateral facet. The hand must also be evaluated for concomitant carpal tunnel syndrome, flexor carpi radialis tunnel syndrome, and DeQuervain tenosynovitis, as these can also need to be addressed. The variety of injections must be limited to a maximum of three; theoretically greater than three injections will increase joint morbidity. After reduction, if the joint remains reduced, the damage may be treated with forged immobilization. If the joint is unstable at all after an attempt at closed discount, surgical administration is indicated. In the presence of articular pathology, arthroplasty could be the remedy of selection, depending on the degree of chondromalacia. In the case of acute trauma, associated fractures and hand injuries must be addressed. The technique presented here is the basic volar ligament reconstruction described by Eaton and Littler. Positioning the process is performed with the affected person supine and the arm on a normal hand table. The working desk must be turned away from the anesthesia machines to allow the surgeon and assistant to sit throughout from each other at the hand table. Once via the pores and skin, care should be taken to keep away from transection of superficial radial sensory nerve branches that may be crossing the operative subject. The radial border of the thenar muscles is incised and elevated, exposing the thumb carpometacarpal joint.
Buy fertomid 50mg without a prescriptionSubchondral surfaces are reinforced with autologous bone graft before cementation xeloda menopause buy cheapest fertomid. In response to these problems women's health clinic ucf generic fertomid 50mg mastercard, closed cryoablation utilizing argon gasoline was developed and have become out there within the late 1990s menstruation occurs when generic fertomid 50mg. This principle of reconstruction is applied in all anatomic locations: proximal femur (A) pregnancy 9 weeks 4 days fertomid 50 mg with mastercard, distal femur (B), proximal tibia (C), distal tibia (D), distal radius (E), and proximal ulna (F). The gel freezes and creates an ice ball inside a couple of seconds after perfusion of the argon fuel through the probe. It would have been troublesome to freeze these websites with direct pour of liquid nitrogen because of the relatively massive measurement of the B funnels. Patients with lesions of the lower extremities are kept non�weight bearing for 6 weeks. Plain radiographs are then obtained to rule out fracture and set up bone graft incorporation. It would have been troublesome to achieve such a range and muscle power after the resection of the distal femur that otherwise would have been supplied to this affected person. This potential drawback initially was underestimated by surgeons who pioneered the appliance of this system in medical apply. Inadequate safety of soft tissues, lack of mechanical fixation, and failure to use perioperative antibiotics resulted in unacceptably excessive rates of fractures, delicate tissue damage, infections, and neurapraxias. As a result, the identical authors reported a later series of sufferers with a considerably lowered price of these issues. They had been thought of pathological because they occurred via a mechanically weakened bone and following a minor trauma. Infections and flap necrosis also have become uncommon issues because of mobilization and safety of soft tissues previous to freezing and the utilization of perioperative antibiotics. When the latter do happen, the neurologic damage usually is transient and heals spontaneously. Cryoablation additionally was proven to be related to minimal injury to the adjoining articular cartilage, with degenerative modifications reported in lower than 3% of circumstances in a big sequence of sufferers. Plain radiograph displaying pathological fracture of the proximal tibia following cryoablation and on weight bearing. Reconstruction following cryoablation in that patient consisted of autologous bone graft solely. The extensive collapse and destruction of the articular floor made resection of the proximal tibia and reconstruction with endoprosthesis inevitable. This complication is uncommon when sufficient padding and warming with saline are carried out. Any compromise of both of these standards ultimately might lead to native tumor recurrence. Better case choice, enough curettage, and meticulous burr-drilling have led to a drop in native recurrence charges, to lower than 5% in most series. Although most of the fuel exits into the ambiance through the surgical wound, a substantial quantity nevertheless is pushed into the pulmonary circulation beneath the affect of the strain caused by boiling of liquid nitrogen in the bony cavity, and exhaled. Treatment of large subchondral tumors of the knee with cryosurgery and composite reconstruction. Recurrent aneurysmal bone cyst of the proximal phalanx treated with cryosurgery: a case report. Tissue impedance and temperature measurements in relation to necrosis in experimental cryosurgery. Effect of hypertonic stress on mammalian cell traces and its relevance to freeze-thaw injury. Cryosurgery in long bones: an experimental research of necrosis and revitalization in rabbits. Cryosurgery and acrylic cementation as surgical adjuncts within the remedy of aggressive (benign) bone tumors: analysis of 25 sufferers below the age of 21.

Generic 50 mg fertomid amexPreoperative Planning With open injuries womens health 6 week ab workout cheap fertomid 50 mg on-line, the surgeon ought to determine if the cause was related to a chunk zinc menstrual cycle safe fertomid 50mg. Sensory branches of the radial or ulnar nerves womens health 6 10 purchase fertomid uk, or both breast cancer 3 day 2015 buy discount fertomid online, are identified and protected. Excess tissue is excised from the realm between the torn sagittal band and the widespread extensor tendon. The sagittal fibers are then repaired using 4-0 or 5-0 nonabsorbable suture (Ethibond). The restore is performed with the joint in 60 to 70 degrees of flexion to keep away from rigidity on the restore and stiffness of the joint. As with all reconstruction techniques, rigidity is set by taking the joint by way of a full vary of motion and documenting stability dorsally. The distally primarily based slip of extensor tendon (black arrowhead) has been rerouted volar to the radial collateral ligament (yellow arrowhead) from a distal to proximal course. The remaining ulnar sagittal band was repaired to stop radial subluxation of the extensor tendon (red arrowhead). Begin proximally by separating the lumbrical muscle from the more dorsal interossei. With the extensor tendon reduced, an isometric point in the extensor tendon should be identified. Tension is set appropriately while gently ranging the finger to affirm the absence of subluxation. Surgical publicity figuring out the extensor dislocation (black arrow) with a big persistent defect within the radial sagittal band (white arrow). The lumbrical muscle�tendon unit is isolated and mobilized for switch (black arrow). This segment of tendon is then handed through a small slit in the remaining tendon on the level of the deep transverse metacarpal ligament to forestall additional propagation of the tendon break up. The slip of extensor tendon is rerouted from proximal to distal, across the deep intermetacarpal ligament. It is then introduced over to the radial facet of the affected finger, nonetheless in continuity with the tendon, and sutured to the palmar portion of the remaining sagittal band after right tension has been set to centralize the tendon. Sometimes the sagittal band, as nicely as the junctura tendinum, on the uninjured side would require release to centralize the tendon. Several postoperative protocols have been described for nondynamic reconstructions. Five had been handled operatively utilizing a slip of extensor tendon looped around the collateral ligament. Watson et al17 described sixteen patients handled operatively with a slip of extensor tendon looped via the deep transverse metacarpal ligament. Hame and Melone 5 reported on eight professional athletes who underwent immediate restore of sagittal band injuries with subluxation of the extensor tendon. With nonoperative therapy, attainable issues embrace joint stiffness, skin irritation from splinting, and failure of therapy. With operative therapy, potential complications include an infection, joint stiffness, injury to neurovascular structures, and failure of remedy with recurrent subluxation or dislocation either in a radial or ulnar path. Posttraumatic ulnar subluxation of the extensor tendons: a reconstructive method. Closed treatment of nonrheumatoid extensor tendon dislocations at the metacarpophalangeal joint. The extensor retinacular system at the metacarpophalangeal joint: an anatomical and histological examine. Dynamic lumbrical muscle transfer for correction of posttraumatic extensor tendon subluxation. Flexor tendons within the carpal tunnel have the added function of subsynovial connective tissue, which may turn into infected. Tenosynovitis is irritation of the tendon sheath in extrasynovial tendons, and irritation of the synovial lining in intrasynovial tendons. The fourth extensor compartment tendons-the extensor digitorum communis and the extensor indicis proprius-lie under a broad retinaculum. The deep department of the posterior interosseous nerve programs deep to the fourth extensor compartment.
|